Surgery to the lymph nodes
Breast cancer cells can sometimes spread to the lymph nodes under the arm.
Most people with invasive breast cancer will have the lymph nodes under the arm assessed. The outcome of this will help the treatment team recommend which treatments are best for you.
The lymph nodes
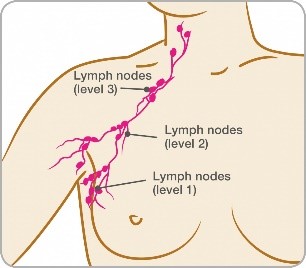
Breasts contain a network of tiny tubes called lymph vessels. These drain into the lymph nodes (glands) under the arm (axilla).
Lymph nodes are arranged in three levels (1, 2 and 3 – as illustrated below). The exact number of nodes in each level will vary from person to person.
Checking lymph nodes before surgery
If you have invasive breast cancer, your treatment team will want to check if any of the lymph nodes under the arm contain cancer cells. This helps them decide whether you’ll benefit from any additional treatment after surgery.
Usually an ultrasound scan of the underarm is done before surgery to assess the lymph nodes.
If this appears abnormal, you’ll have a fine needle aspiration (FNA) or a core biopsy to see if the cancer has spread to the lymph nodes. An FNA uses a fine needle and syringe to take a sample of cells to be looked at under a microscope. A core biopsy uses a hollow needle to take a sample of tissue for analysis under a microscope.
Lymph node removal
If the FNA or core biopsy shows cancer has spread to the lymph nodes, you’ll usually be recommended to have all or most of your lymph nodes removed. This will be done at the same time as your breast surgery and is known as an axillary clearance.
Sentinel lymph node biopsy
If you have invasive breast cancer, even if the radiology tests before surgery show no evidence of the lymph nodes containing cancer cells, you will usually still need to have a sentinel lymph node biopsy during surgery.
Sentinel lymph node biopsy is used to identify whether the sentinel lymph node (the first lymph node that the cancer cells are most likely to spread to) is clear of cancer cells. There may be more than one sentinel lymph node.
Sentinel lymph node biopsy is usually carried out at the same time as your cancer surgery but may be done before.
There are two ways we can identify the first node(s) to drain the breast: using nuclear medicine (radioisotope) or Magtrace (an iron nanoparticle).
A small amount of the tracer is injected into the area around the cancer to identify the sentinel lymph node. Once removed, the sentinel node is examined under a microscope to see if it contains any cancer cells.
If the sentinel node does not contain cancer cells, this means the other nodes are clear too, so no more will need to be removed.
If the results show there are cancer cells in the sentinel node, depending on how much is found you may be recommended to have:
- further surgery to remove some or all of the remaining lymph nodes
- radiotherapy to the underarm
- no further treatment to the underarm as long as you are having radiotherapy to the breast and chemotherapy or hormone therapy treatment
For patients thought to have DCIS or non invasive cancer that requires a mastectomy, Magtrace can be used in a delayed setting. The 30-day injection window means that some DCIS patients could avoid unnecessary lymph node surgery, as surgery only needs to proceed after pathology has confirmed there is a benefit in doing so. In these cases Magtrace is injected in the operating theatre.
Isolated tumour cells (ITCs), micrometastases and macrometastases
Your doctor may use one of these terms when discussing your sentinel lymph node biopsy result.
- ITCs are single cancer cells or small clusters of cells no bigger than 0.2mm.
- micrometastases are cancer cells larger than 0.2mm but not bigger than 2mm.
- macrometastases are cancer cells larger than 2mm.
If you’re diagnosed with ITCs or micrometastases, you will not usually need any further treatment to your axilla (under the arm).
If you have one or two sentinel nodes with macrometastases, you may or may not need further treatment to your axilla. This will depend on several factors including other characteristics of the cancer, for example what the grade is and whether you’re having hormone therapy. Your doctors may talk about further surgery or radiotherapy to the axilla. On some occasions no further treatment may be appropriate.
If you have three or more sentinel nodes with macrometastases, you will need further treatment to the axilla.